Events Report by Committee
Here's another simple report that has much potential to help improve the case identification process.
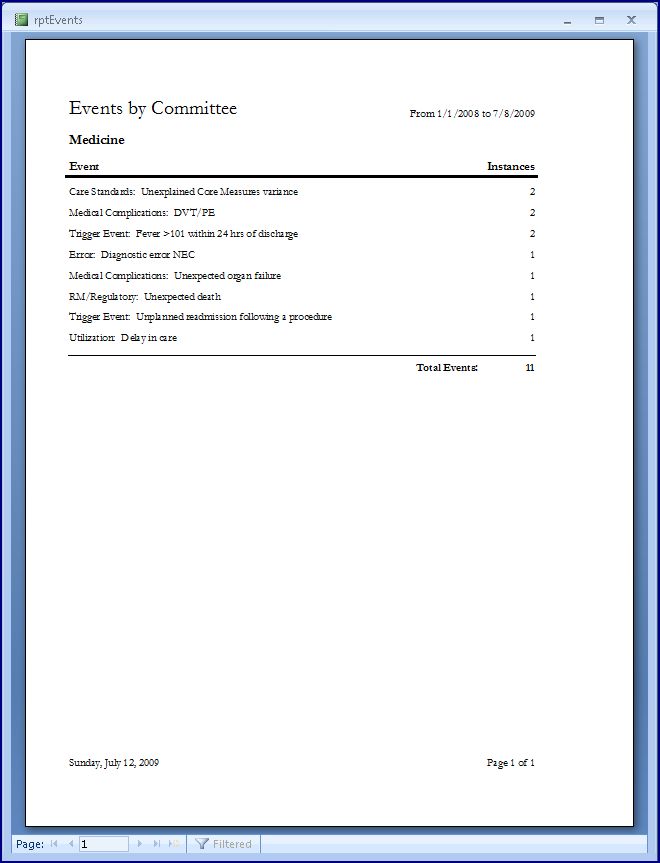
It answers the question, "What have we been looking at?"
In this mock example (disregarding case volume), we note the relative absence of cases of readmission. I find that many medical review committees do little else than review readmissions. The literature shows that readmission for medically treated patients may have reasonable sensitivity for substandard care, but very low specificity. The result is that review of readmissions is not much better than random case review (at least when looking for substandard care).
The point here is that exclusive reliance on a single trigger for case review suggests a problem with identification of other types of potential learning opportunities.
Please note that substandard care per se is not the target of the QI Model. My reseach has demonstrated that focus on the presence or absence of substandard care is dysfunctional and is a prime contributor to the persistence of a culture of blame. In contrast, the best-practice QI Model looks more broadly for all types of learning opportunities in the system of care.